REVISIÓN
Indications and decision making in single and multiple treatment of the anterior sector
Indicaciones y toma de decisiones en el tratamiento unitario y múltiples del sector anterior
Ianina Solange Silvera1, Natalia Argenio1*, Hugo Parco Valiente1*, Maria Isabel Brusca1*
1Universidad Abierta Interamericana. Buenos Aires, Argentina.
Cite as: Silvera IS, Argenio N, Parco Valiente H, Brusca MI. Indications and decision making in single and multiple treatment of the anterior sector. Odontologia (Montevideo). 2024; 2:122. https://doi.org/10.62486/agodonto2024122
Submitted: 02-02-2024 Revised: 13-05-2024 Accepted: 28-08-2024 Published: 29-08-2024
Editor: Nairobi
Hernández Bridón ![]()
ABSTRACT
Gingival recessions, characterized by apical displacement of the gingival margin and exposure of the root surface, pose both esthetic and functional challenges. This paper reviews the indications and decision making in the management of anterior gingival recessions, a crucial aspect in esthetic and restorative dentistry. Over the years, the evolution of mucogingival surgery towards periodontal plastic surgery has led to the development of various surgical techniques, such as connective tissue grafts and advanced coronal flaps. These techniques aim to provide effective and durable root coverage, adapting to the specific anatomical characteristics of each patient. The selection of the most appropriate surgical technique depends on a detailed evaluation of local anatomical factors and the patient’s esthetic expectations. While it is possible to maintain periodontal health with a minimal amount of keratinized gingiva, gingival recessions remain common, especially in individuals with thin periodontal phenotypes. An interdisciplinary approach is essential to ensure outcomes that optimize both periodontal health and esthetics in the long term.
Keywords: Gingiva; Periodontics; Tissue Regeneration; Congenital Anomalies; Esthetics.
RESUMEN
Las recesiones gingivales, caracterizadas por el desplazamiento apical del margen gingival y la exposición de la superficie radicular, plantean desafíos tanto estéticos como funcionales. El presente trabajo revisa las indicaciones y la toma de decisiones en el manejo de recesiones gingivales en el sector anterior, un aspecto crucial en odontología estética y rehabilitadora. A lo largo de los años, la evolución de la cirugía mucogingival hacia la cirugía plástica periodontal ha permitido desarrollar diversas técnicas quirúrgicas, como los injertos de tejido conectivo y los colgajos avanzados coronales. Estas técnicas buscan proporcionar una cobertura radicular efectiva y duradera, adaptándose a las características anatómicas específicas de cada paciente. La selección de la técnica quirúrgica más adecuada depende de una evaluación detallada de factores anatómicos locales y de las expectativas estéticas del paciente. Si bien es posible mantener la salud periodontal con una cantidad mínima de encía queratinizada, las recesiones gingivales siguen siendo frecuentes, especialmente en individuos con fenotipos periodontales delgados. El enfoque interdisciplinario es fundamental para garantizar resultados que optimicen tanto la salud periodontal como la estética a largo plazo.
Palabras clave: Encía; Periodoncia; Regeneración Tisular; Anomalías Congénitas; Estética.
INTRODUCTION
Mucogingival disorders are acquired alterations in the morphology, position or amount of gingiva surrounding the teeth, among which we can include gingival recessions, which are defined as the apical displacement of the gingival margin beyond the amelocementary line with exposure of the root surface, which can affect one or more teeth.(1)
Nowadays, these alterations are an integral part of esthetic and rehabilitative dentistry. Patients are frequently concerned about the appearance of the teeth with the soft tissues, one of the most common being recession. Although esthetic compromise is usually the main reason for consultation, so are tooth sensitivity, caries and cervical lesions.(2)
Trends and networks lead to high demands when establishing esthetic parameters, forcing professionals to develop new techniques and procedures to achieve predictable and long-lasting results in an effective and long-term manner. During the last 30 years, surgical techniques have been proposed to treat single and multiple gingival recessions, using displaced flaps, free grafts, bilaminar techniques, or even regenerative procedures using guided tissue regeneration techniques or enamel matrix derivatives.(3)
Despite the above, the intention to modify or treat soft tissue conditions dates back a long time. The term mucogingival surgery began in 1957 by Nathan Friedman and was later complemented by periodontal plastic surgery in 1993 by Dr. Miller. Establishing it as a speciality in periodontics in 1990. The beginnings of mucogingival surgery were the use of free grafts and the treatment of aberrant frenulum or alterations that extend beyond the mucogingival line.(4)
There are multiple classifications for identifying recessions, each describing a specific area. For example, Miller’s classification seeks to predict the success of root coverage, similar to Cairo’s intention. In contrast, Pini and Prato’s classification evaluates whether or not the need for reconstruction of lesions at the amelocemental boundary is necessary.(5,6,7)
On the other hand, the American Academy of Periodontology and the European Federation of Periodontology, in the current classification of periodontal and peri-implant diseases and disorders, mention mucogingival deformities establishing parameters that modify the gingival tissue: these include periodontal phenotype, presence of gingival recession, lack of keratinized gingiva, gingival excess, alterations of exposed root surfaces, among others. This way, it guides decision-making for better performance and therapeutic action.(8)
On the other hand, the percentages of veneering vary according to the anatomical conditions of the sector or the tooth/pieces to be treated, as well as the type of recession the patient has, presence of muscular insertions, shallow depth of the vestibule, root prominence, narrow papillae, etc.; therefore, the selection of one technique instead of another depends on the anatomical characteristics of the location to be treated and the patient’s demand.(9)
This work intends to consider the clinical parameters, articles, and techniques described for a better approximation in the decision-making process for treating single and multiple gingival recessions.
METHOD
The following work refers to a theoretical discussion, conducting the research through a bibliographic search of scientific articles in the last ten years in different digital databases such as Scielo, Medline, Lilacs, Pubmed, Google Scholar, digital libraries, in English and Spanish languages using the following descriptors: “mucogingival alterations”; “gingival recessions”; “multiple recessions”; “free graft”; “connective tissue graft”, “coronal displaced flaps”; “gingival recession coverage”.
Books on the subject will be used to describe the gingiva periodontal complex in the teeth.
Inclusion criteria:
· Scientific articles of patients treated with a diagnosis of single or multiple gingival recessions.
· Any type of research study will be valid (clinical practice, clinical trial, observational study, clinical trial).
Exclusion criteria:
· Articles that do not report clinical data.
· Articles referring to orthodontic and orthognathic treatments related to recessions, laser treatments, iatrogenic considerations, endoperiodontal relations, hyaluronic acid treatments.
From a total of 521 articles, 190 were selected that met the inclusion criteria for the literature review.
RESULTS AND DISCUSSION
Historical background
Periodontics as a science was founded in 1946, which gave rise to the first Society of Periodontics in Latin America. Years later, in 1986, the glossary of terms established its definition as a branch of dentistry that diagnoses and treats diseases and conditions of the tissues that support and surround the tooth, as well as its substitute implants. Later, in 1993, it was defined as a speciality within dentistry, comprising the prevention, diagnosis and treatment of diseases of the tissues surrounding and supporting the tooth and its substitutes and the maintenance of health, function and esthetics of these structures and tissues.(9,10) This is how it has evolved, establishing its importance for daily practice.
Periodontics today, called “the conscience of dentistry”, is present in the various specialities because it has unquestionable relationships with the other areas of the profession; however, as a differentiated specialization, it may seem young about other specialties.(10)
The 2017 classification of periodontal and peri-implant diseases and alterations summarizes the health considerations, disease and gingival alterations observed on dental pieces and their substitutes. Gingivitis is defined as gingival inflammation and the absence of detectable clinical attachment loss due to previous periodontitis. A case of periodontitis is established when interdental clinical attachment loss is detected in at least two or more non-adjacent teeth or clinical attachment loss is detected in free faces greater than or equal to 3 mm with a probing depth greater than 3 mm as long as the clinical attachment loss is not due to situations other than periodontitis.(8)
Since it began with Dr Fermín Carranza in 1934, treating periodontal alterations has required surgical complementarity, most with respective techniques.(10) In 1964, Dr. Nathan Friedman began to show interest in preserving the condition of the soft tissues surrounding the tooth using mucogingival techniques.(11) A few years later, Dr. Preston Miller 1993 introduced periodontal plastic surgery, which seeks to prevent or correct anatomical problems and developmental, traumatic or disease-induced defects of the gingiva, mucosa or alveolar bone.(5)
DEVELOPMENT
The gingival margin is clinically represented by a scalloped line that follows the contour of the amelocemental junction.(12) Gingival recession is an apical displacement of the gingival margin with exposure of the root surface to the oral cavity.(4,6,9)
The American Academy of Periodontology glossary defines gingival recession as “apical migration of the gingival margin beyond the cemento-enamel junction.”(6)
Mucogingival disorders are acquired alterations of the morphology, position or amount of gingiva surrounding the teeth, within which we can locate gingival recessions, which can affect one or more teeth.(1,13) They are commonly located on the vestibular surfaces, although it is also possible to locate them in the palatal and lingual areas less frequently.(9)
The modifications that affect the gingival tissue include periodontal phenotype, gingival recessions, lack of keratinized gingiva, gingival excess, and alterations of the exposed root surfaces. Thus, the new classification guides decision-making for better performance and therapeutic action.(8)
Periodontal phenotype refers to the combination of gingival phenotype and bone morphotype. The former indicates the three-dimensional gingival volume, while the latter establishes the thickness of the bone table. The definition of phenotype accounts for the appearance of an organ based on the multifactorial combination of genetic traits and environmental factors, including, in the same term, the genetic biotype of the organ in question. Thus, the phenotype indicates a dimension that may vary over time depending on environmental factors and clinical intervention and is site-specific and independent.(8)
The distinction between the different phenotypes is based on the anatomical characteristics of the components of the periodontium, including gingival thickness (GT), keratinized tissue width (KTW) and bone morphotype (BM). It has been reported that the thin phenotype is associated with GT ≤1mm, KTW between 2,75 - 5,44mm, setting the average at 4,15mm and BM 0,343 mm, while the thick phenotype is associated with GT >1mm. KTW between 5,09 - 6,65mm, determining the average at 5,72mm and BM at 0,75mm.(14,15)
Among mucogingival deformities, lack of keratinized tissue and gingival recession are the most common. A recent consensus concluded that no minimum amount of keratinized tissue is necessary to prevent attachment loss when good conditions exist. However, the attached gingiva is essential for maintaining gingival health.(15)
Aetiology
In many cases, the diagnosis is determined during the clinical inspection in the dental office. However, in other cases, the patients reconsider the appearance of the teeth and soft tissues, expressing their concern to the professionals about the presence of an alteration. Although esthetic compromise is usually the main reason for consultation, so is tooth sensitivity, caries and cervical lesions.(2,4,9,16)
An extensive literature search revealed the following findings: 1) periodontal health can be maintained in most patients with routine dental consultation; 2) thin periodontal phenotypes are at increased risk of developing gingival recession; 3) oral hygiene, orthodontic treatment, and inadequate cervical restorations may increase the risk of developing gingival recession; 4) surgical intervention, either to change the phenotype and to cover roots, may be indicated when the risk of development or progression of pathology and associated root damage is increased and to meet the esthetic requirements of patients.(15)
Although the aetiology of gingival recession remains unclear, several predisposing and triggering factors have been suggested, including brushing trauma, dental malposition, the presence of restorations and cervical lesions, inadequate oral hygiene, orthodontic movements, braces traction, persistent gingival inflammation and periodontal phenotypes.(4,9,14,17)
The impact of improper tooth brushing was evaluated during a systematic review, and the results were inconclusive. Some studies concluded that toothbrushing reduced recessions on facial surfaces, while others concluded that there appeared to be no relationship between brushing frequency and gingival recessions. In contrast, others reported a positive association between frequency and recessions. All reported risk factors during brushing, such as duration, brushing strength, frequency of brush change, brush bristle hardness and brushing technique.(9,18) Following this axis, trauma from improper flossing may contribute to the gingival lesion, which is characterized as deep and narrow, similar to a “Stillman’s Fissure”. The initial lesion may appear as a linear V-shaped ulcerated cleft with edematous borders showing a red surface, reversible as long as flossing is discontinued. However, if the indentation appears white, the gingival lesion is irreversible.(9)
The position of the teeth in the alveolar process affects the amount of gingiva inserted around the tooth, with variation in gingival width, keratinized tissue width and bone morphotype. The buccal or vestibular position of the teeth is frequently associated with thin phenotypes.(9,15)
On the other hand, the gingival recession may initiate or progress during or after orthodontic treatment, depending on the direction of movement. Some investigators claim that gingival recession is associated with labial movement; however, when a vestibulolingually positioned tooth is moved lingually, the dimension of the tissues in its vestibular portion will increase in width.(9,15,19)
A thin periodontal phenotype, the absence of keratinized tissue and reduced alveolar bone thickness due to the position of the teeth in the arch is considered an anatomical risk factor for the development and progression of gingival recessions, including the presence of fenestrations or bony dehiscences. In correlation with tissue characteristics, individuals with thin phenotypes have narrow and long teeth. They are more prone to recession compared to those with a thick phenotype, where individuals have short and wide teeth.(9,15,20)
Sites with minimal or no gingiva associated with restorations close to the cervical areas are more prone to gingival recession and inflammation. The authors concluded that gingival augmentation is indicated for these clinical situations.(15)
Current consensus considers the presence of about 2mm width and about 1mm gingival thickness, together with optimal plaque control, necessary for maintaining gingival health.(15)
Cervical non-carious lesions (CNCL) are modifications of the root surfaces with the potential disappearance of the amelocemental junction and formation of steps of different depths and extents depending on their aetiology. Different studies reveal the high prevalence of NCCLs with recession.(15)
Epidemiology
Mucogingival defects, including gingival recession, occur frequently in adults and tend to increase with age, occurring in populations with high and low oral hygiene standards.(13,15) Their incidence ranges from 8 per cent in children to 100 per cent after age 50.(17)
A 2003 study revealed that 88 per cent of people aged 65 years and older and 50 per cent of people aged 18 to 64 years have one or more sites of gingival recession. They also found that the prevalence of a recession of 1 mm or more in people 30 or older was 58 per cent and increased with age. Men and African Americans had significantly more gingival recession than women and other racial/ethnic groups, respectively.(18)
Recession was also more frequent and severe on the vestibular surfaces than on the interproximal areas of the teeth. Similarly, the frequency of gingival recession increased with age and was higher in men than in women of the same age.(13,21)
The results of the systematic review and meta-analysis conducted between 1991 and 2021 from five electronic databases and hand searches aimed to estimate the general population’s overall prevalence of gingival recession. A total of 15 studies with 37460 participants were included, and it found that more than two-thirds of the world’s population was affected by gingival recession.(22)
Ranking
The classifications of gingival recessions are multiple, and each one describes a specific area of great importance since they determine a way of organizing knowledge and justifying the decision-making process when choosing a procedure.(9,16,23)
The reason for many classifications is diverse; some remain unchanged over time, and others seek to incorporate new knowledge.
In chronological order, we find Sullivan and Atkins (1968), Miller (1983), Pini Prato (2010) and Cairo (2011).(5,6,7,24) In this work, we will analyze the Miller and Cairo classifications as they are the most widely used in the literature.
Sullivan and Atkins (1968) classified gingival defects into four morphological categories: superficial-narrow, superficial-wide, deep-narrow and deep-wide.(18)
Miller (1985) proposed four types of gingival recessions based on the height of the gingival margin concerning the mucogingival junction and the level of the underlying alveolar bone.(5,25)
· In class I gingival recession does not reach the mucogingival junction and there is no interproximal bone loss.
· In class II gingival recession extends to or beyond the mucogingival junction and there is no interproximal bone loss.
· In class III gingival recession reaches the mucogingival junction and there is interproximal bone loss.
· In class IV gingival recession extends to or beyond the mucogingival junction and there is severe interproximal bone loss.
In addition, Miller proposed the prognosis or viability of root coverage for each classification. For classes I and II, total coverage is established; for class III, partial coverage and no root coverage for class IV.(5,9,25)
Pini and Prato 2010 proposed a clinical classification of surface defects in teeth associated with gingival recession. They identified four classes of tooth surface defects in areas of gingival recession based on the presence (Class A) or absence (Class B) of the amelocemental junction and the presence (Class +) or absence (Class -) of surface discrepancy.(6,9) This evaluates the need for reconstruction or not of lesions at the amelocemental-cemental boundary prior to the surgical stage.(24)
Cairo describes a system for classifying gingival recession defects into three types, considering the level of clinical interproximal attachment. In addition, he establishes a prediction of the final results of root coverage according to the type of gingival recession.(7,9)
In recession type 1 (RT1), there is no interproximal attachment loss, and clinically, the amelocemental junction at the interproximal level is not detectable mesially and distally of the tooth.
Recession type 2 (RT2) is associated with interproximal attachment loss. The amount of interproximal attachment loss (measured from the interproximal cement-amelocemental junction to the interproximal pocket depth) is less than or equal to the buccal attachment loss (measured from the vestibular cemento-amelocemental junction to the vestibular pocket depth).
Gingival recession type 3 (RT3) is associated with interproximal attachment loss but is more significant than buccal attachment loss.
Clinical diagnosis
The clinical elements to be considered for the orientation of the treatment are the depth and type of recession the patient has, the presence of muscular insertions, the shallow depth of the vestibule, the root prominence, the dental position, the level of clinical interdental insertion, the phenotype, the amount of gingival tissue, the history of root coverage surgery and the esthetics of the site, which conditions the success of the root coverage surgery; Therefore, the selection of one technique over another depends on the anatomical characteristics of the site to be treated and the patient’s demand.(9,26)
The predictability of root coverage estimates the percentage of exposed root surfaces that can be covered with soft tissue. For the correct evaluation of this parameter, it is necessary to recognize the cementoenamel junction of the tooth or teeth that are affected. When the cementoenamel junction is not recognizable, it is no longer possible to measure the depth or width of recession and thus evaluate the efficacy of a surgical technique regarding root coverage due to the lack of the reference parameter.(9)
Root percentage refers to the amount of root surface covered by gingiva. It is expressed as a percentage and is used to assess the periodontal health of a tooth, with the gingiva ideally covering at least 85 % of the root surface for good periodontal health. On the other hand, root coverage refers to the surgical procedure performed to increase the gingiva covering the exposed root surface. Therefore, the clinical healing pattern can only be determined in those gingival recessions where the amelocemental junction is clinically detectable and can be evaluated in percentage and complete root coverage.(9,13,16,23)
The ideal papilla height in a tooth with gingival recession was defined as the apicocoronal dimension of the interdental papilla capable of supporting complete root coverage. The ideal papilla height was measured as the distance between the point where the cementoenamel junction crosses the mesial-distal facial line angle of the tooth, called the angular point of the cementoenamel junction and the point of contact. The angular point of the cementoenamel junction is easily identifiable, even in a tooth with non-carious cervical lesions. Once the ideal papilla was measured, this dimension was replicated apically, starting from the tip of the mesial and distal papillae of the tooth with the recession defect. Horizontal projections at the margin of recession from these measurements allowed the identification of two points connected by a scalloped line, representing the ‘root coverage line’.
Therefore, the most important prognostic factor for root coverage after surgery is the height of the interdental periodontal support.(22,23,26)
Surgical techniques
During the last 30 years, surgical techniques have been proposed to treat single and multiple gingival recessions, using displaced flaps, free grafts, bilaminar techniques, or even regenerative procedures using guided tissue regeneration techniques or enamel matrix derivatives.(7,9,13,16,27)
The term mucogingival surgery, introduced by Friedman in 1957, is applied to surgical procedures used to solve problems related to the interrelationship between the gingiva and the alveolar mucosa, designed to preserve gingival tissue, such as pockets extending apically to the mucogingival junction, malposition of the frenulum and inadequate vestibular depth.(11) For that reason, in 1993, Miller introduced the term periodontal plastic surgery, which is defined as surgical procedures performed to prevent or correct anatomic, developmental, traumatic or disease-induced defects of the gingiva, alveolar mucosa or bone. This definition was accepted by the international scientific community in 1996 and includes various soft and hard tissue procedures for gingival augmentation, root coverage, correction of mucosal defects in implants, crown lengthening, gingival preservation in ectopic tooth eruption, removal of aberrant frenular, prevention of ridge collapse associated with tooth extraction, and edentulous ridge augmentation.(9,16)
A single gingival recession occurs when only one tooth in the arch is affected. The probable cause is factors such as overly vigorous tooth brushing, tooth malposition, or local trauma such as perioral perforations.(9,16) Features present in single gingival recessions include:
· Loss of gingival tissue in a single tooth or gingival area.
· Exposure of the tooth root.
· Tooth sensitivity.
· Aesthetic alteration of the smile.
· Increased risk of periodontal disease.
Multiple recessions are observed when gingival recession affects several teeth in different mouth areas. Among the associated causes, we can mention orthodontic movements, occlusion problems, and periodontal disease.(9,16) Clinical features in multiple gingival recessions include:
· Loss of gingival tissue in multiple teeth or gingival areas.
· Exposure of multiple tooth roots.
· Widespread tooth sensitivity.
· Aesthetic alteration in multiple areas of the smile.
· Increased risk of periodontal disease in various areas of the mouth.
Epithelialized Palatal Graft (EPG) / Free Gingival Graft (FGG)
The use of free gingival grafts in periodontal therapy was first described by Bjorn in 1963 to create a wider area of inserted gingiva. However, interest in palatal mucosal grafting began with Nabers’ work on this technique to deepen the buccal sulcus.(28,29,30) Sullivan and Atkins described the technique in 1968, and it was subsequently modified by Miller in 1982.(27)
The surgical steps to perform the technique are as follows:(29)
A. A partial thickness flap is prepared in the recipient area, extending 5mm apically beyond the bone dehiscence and mesiodistally reaching one more tooth on each side of the area to be treated. The incision will be horizontal, with the scalpel blade oriented perpendicularly to the base of the papillae, looking for a good adaptation between the graft and the base of the papillae and a correct vascularization of the donor tissue. At both ends of the horizontal incision, two parallel vertical incisions extend apically, reaching the mucogingival line; the gingiva is partially dissected until a receptor bed is obtained.
B. Root surface preparation with curettes: The surfaces are conditioned by removing calculus and root cement. A surgical template is made with the dimensions of the graft to be taken.
C. On the palate, with the support of the template, the dimensions of the graft are traced in the premolar area with a safety margin of 2-3mm from the gingival margin, removing the epithelialized graft with a thickness of 1,5mm and depositing it in saline solution to avoid its dehydration.
D. The graft is adapted in the recipient area and fixed with simple sutures in the area of the papillae and suspensory or cross sutures that compress and stabilize the donor tissue on the bed. The operated region is protected with surgical cement. Antibiotic therapy is indicated, and the sutures are maintained for 10 to 14 days, after which the cement and sutures are removed
Free gingival grafting for root coverage is a one-stage, highly predictable procedure, regardless of the quality or quantity of gingival tissue adjacent to the recession. Its main indication is to increase the amount of attached gingiva to allow proper hygiene, although it should be used with caution in esthetically sensitive areas due to the inconsistent colour mixing of the graft concerning the gingival tissues, as well as the expected 40 % shrinkage.(28,31)
Connective Tissue Graft (CTG) / Bilaminar Technique
Since the mid-1990s, clinicians have introduced several modifications to the original bilaminar procedure described by Raetzke. He created a trapdoor flap in the palate to harvest a connective tissue graft placed coronally between a partial thickness and underlying periosteum.(29) His design proposes several advantages over epithelialized or free grafting, including increased blood supply to the graft through intimate contact with the surrounding tissues, a reduced tendency for graft shrinkage, and more aesthetic colour integration in the operated area.(27,30,32,33)
The surgical method used consists of the following steps:
1. A collar of tissue, whose width corresponds to the depth of the sulcus, is removed from the receded gingiva to remove the sulcus epithelium.
2. The affected tooth’s root is carefully scraped and brushed until its surface is smooth and hard. Citric acid is applied to its surface.
3. An undermined partial-thickness incision creates an “envelope” or “envelope” in the tissue around the bare root surface.
4. In the premolar/molar region of the palate, close to the teeth, two incisions are made 1 to 2 mm apart in the anterior/posterior direction. Their length should be equal to twice the width of the recession area. They are carried deep into the palatal mucosa, where they converge just anterior to the bone.
5. A portion of tissue is removed, and its small band of epithelium is excised. Epithelium may be left in the medial part of the graft, which remains on the exposed root.
6. The graft is placed in the previously created lobe envelope to completely cover the previously exposed root area. Finger pressure is applied with gauze until the bleeding stops and the graft is firmly seated. It is then secured with an adhesive tissue, and sutures are required. The area is covered with a periodontal dressing without eugenol for one week.
7. In the donor site, the wound edges are adapted with sutures. Due to the small extent of the superficial defect, no additional protection is necessary.
In 1985, Langer and Langer described the use of subepithelial connective tissue grafting as a procedure to increase the amount of keratinized gingiva and to achieve root coverage. They designed a technique consisting of a rectangular incision with two horizontal and two vertical incisions.(27,34,35)
Harris, in 1992, proposed two surgical techniques: the method of free gingival grafting with a blade in which a partial-thickness flap is made by pushing the scalpel blade under control distally through the palate and the method of parallel incisions through a single incision with a double blade scalpel to take a 1,5 mm thick graft with an epithelial margin.(36)
Bruno, in 1994, performed the harvesting of the donor tissue with a first incision in the palate perpendicular to the longitudinal axis of the teeth, approximately 2 to 3 mm apical to the gingival margin of the maxillary teeth. The mesiodistal length of the incision is determined by the graft length required for the recipient site. The second incision is made parallel to the longitudinal axis of the teeth, 1 to 2 mm apical to the first incision, depending on the graft thickness required. The incision is made apical to provide sufficient connective tissue height to cover the recipient site’s denuded root and adjacent periosteum. A small periosteal elevator is used to elevate a full-thickness periosteal connective tissue graft.(37)
In 1999, Hürzheler used an incision parallel to the gingival margin to access the donor site. Harvesting of the graft in size and thickness can be obtained without removing any epithelial bands with the connective tissue, and the palatal donor site can be healed with first intention. The length of this incision corresponds to the purpose for which the graft is intended, with a blade angle of 90 degrees to the bone. After the first incision, the bevel of the scalpel blade has an angle of approximately 135 degrees and an undercut preparation is started inward from the first incision; with each new movement of the scalpel along the incision line, the angle is flatter until the blade reaches a position almost parallel to the bone surface. Partial thickness preparation can be observed from outside the tissue outward by attempting to elevate the tissue as the instrument advances. No vertical incisions will be made. This procedure aims to create a partial-thickness mucosal flap with a thickness of 1 to 1,5 mm, depending on the needs of the recipient site.(38)
In 2010, the author, Giovanni Zucchelli, conducted a randomized controlled clinical trial in which root coverage treatment was performed in 50 patients. In the control group, the connective tissue graft was harvested using the trap door technique, while in the test group, a free gingival graft was harvested and subsequently de-epithelialized. Both types of grafts were effective in root coverage for treating gingival recession. A more significant increase in gingival width was achieved in the test patients; this may be due to the better postoperative stability of the connective tissue resulting from the de-epithelialization of the free gingival grafts.(34,39)
Carranza, in 2020, proposed a modified double-scalpel technique. It combines the single-incision technique and the double-bladed scalpel to harvest grafts at a depth compatible with a bilaminar nature. The superficial side includes part of the denser area of the lamina propria, while the deeper side includes a more excellent connective and vascular tissue content.(40)
Factors influencing the choice of technique for soft tissue graft procurement include the donor site’s anatomic characteristics, the graft’s quality and histology obtained, the technique’s simplicity, postoperative complications, operator experience, patient preferences or inherent factors, and clinical outcomes.(34)
The anatomy of the palatal vault can be classified as flat, medium or high. Therefore, it is imperative to define a safety zone for harvesting connective tissue grafts.(35,41)
Tavelli et al. identified by computed tomography the position of the posterior palatal foramen (PPP) and the position of the palatal artery (PA), being on average 7, 12 and 17 mm from the cementoenamel junction of the maxillary teeth when the vault is shallow, medium and high, respectively.(42)
The location of the APP was estimated to be on the middle and palatal side of the third molar in 57,1 % of cases and between the second and third molar in 21,3 %. In addition, the average distance between the APP and the inter-incisive foramen was 35,8mm. In comparison, the distance between the APP and the posterior border of the hard palate was 3,8mm, and the median suture was 15,2mm respectively. No significant differences were found between males and females.(37)
The diameter of the PA was found to be greater in the molar area and gradually decreases as it approaches the anterior area, except in the second premolar, where it tends to increase. The proposed safety zone indicates the distance from the amelocemental border to the PA, including 2mm of free gingiva in patients with intact, healthy periodontium. However, these references may not be valid in patients with attachment loss or edentulous areas, and other reference points may be necessary.(42)
The palatal mucosa comprises three histologic layers: the epithelium, the subepithelial connective tissue with the lamina propria, and the submucosa. Age, sex, and population characteristics have been reported to be factors that may affect the thickness of the palatal mucosa. The thickness of the masticatory mucosa has been evaluated in different studies. It has been determined that the thickness in the tuberosity area was more significant than 4mm, and in the palatal region, it was an average of 3mm. (35,43)
The area of ortho keratinized epithelium was similar in both regions; the subepithelial connective tissue area and the basal lamina area are well vascularized with small vessels distributed among the collagen fibres and in-depth the submucosal tissue with adipose and glandular cells. However, the most significant difference is that the tuberosity grafts have a higher percentage of lamina propria and less submucosa.(42,44) In summary, grafts from different donor sites appear to have characteristics that may require a selective clinical application based on clinical evidence and depend on the amount of tissue available at the donor sites.(35)
Common postoperative complications include pain and bleeding from the donor site. Zuchelli et al., in their study of patient morbidity after harvesting connective tissue grafts and free grafts, concluded that operative time was significantly shorter for the test group, which correlated significantly with analgesic consumption and that consumption increased as operative time was prolonged. Similarly, both groups reported limited postoperative morbidity.(39)
Coronally positioned flap / Coronally Advanced Flap (CAF)
The coronal advancement flap is a technique that has evolved, having its beginnings in 1985 by Langer and Langer.(27) Allen and Miller 1989 modified including two releasing incisions that start from an apical area to the apex of the anatomical papilla to raise a partial thickness flap along its entire length, being indicated for treating shallow recession.(32) In 1992, an update by Pini and Prato included horizontal incisions and vertical releasing incisions combined with using a Gore-Tex membrane to perform partial thickness in the papillae area.(24)
Finally, Zucchelli and De Sanctis in 2000 combined the techniques described above by making a partial - full - partial thickness flap with de-epithelialization of the anatomical papillae and reconfiguration of the surgical papillae to allow a correct approximation of these at the time of coronal repositioning of the flap.(45)
The described technique is the most appropriate in patients with high esthetic expectations since it provides the best results; it is one of the most studied and predictable flaps for treating unitary recessions. It is indicated when the height of the keratinized tissue apical to the root exposure is > 2 mm. However, some anatomical factors limit its applicability and clinical efficacy. Among them, we mention the absence or minimal amount (≤1 mm) of keratinized tissue apical to the recession defect, the presence of loss of clinical interdental attachment, the presence of a gingival cleft extending into the alveolar mucosa, the presence of high frenulum at the soft tissue margin, profound loss of root structure, root positioned vestibular, and decreased vestibular depth.(9)
According to the literature, it provides 70-80 % root coverage. The step-by-step procedure is as follows:
1. Measure the recession from the gingival margin to the LAC.
2. Horizontal incisions with a minimum extension of 3mm at an apical distance from the apex of the papilla equivalent to the recession +1mm. In this way, we can obtain our surgical papillae.
3. Slightly divergent releasing incisions are bevelled to avoid generating scars and partial thickness along their entire length.
4. Once our surgical papillae have been raised to partial thickness, we use the periosteal tape to make the total thickness, taking advantage of the entire thickness of the flap, and we extend apically with this total thickness up to the equivalent of the recession + 1mm.
5. Confection of the deep partial thickness, with the scalpel parallel to the bone plane, so that we are going to leave a thin layer of periosteum, and we first uninsert the mucogingival line and then the submucosa with all the periosteal flap.
6. Access to the superficial partial thickness is needed to achieve muscle dissection by changing the direction of the scalpel parallel to the flap.
7. Once the flap is free of tension, we perform the root smoothing and de-epithelialize the anatomical papillae that will serve as a vascular bed to anchor the surgical papillae by suturing.
The coronal repositioning flap for multiple recessions perfectly adapts the surgical papilla to the anatomy, eliminating the vertical releasing incisions and allowing the approach to be done in a single surgical act. The design can take two forms depending on the anterior or posterior sector. In the first case, the centre of rotation is the inter-incisive papilla, maintaining its insertion. In contrast, in the second case, the centre of rotation is located at the level of the canine or the highest recession to be covered.(46,47)
Step-by-step planning:
1. Measure the recession of the tooth that will be the centre of rotation from the LAC to the gingival margin.
2. Add 1mm to the height obtained and transfer the measurement as a line from the tip of the papilla parallel to the gingival margin.
3. Measure the distal adjacent recession and transfer the measurement distally.
4. Measure the mesial adjacent recession and transfer the mesial measurement.
5. These measurements indicate the distance of the oblique paramarginal incisions converging towards the centre of rotation, in this example, the canine.
6. If the distal tooth has no recession, the initiation would be horizontal, not achieving an appropriate adaptation and design. To avoid this, a false recession is planned by vertically making the incision and separating the area of the intervention.
7. Lift the partial, total, and partial flap.
8. De-epithelialize the papillae.
9. Reposition the flap up to 1mm coronal to LAC.
Pedicle Flaps
The first approach to laterally displaced flap-making dates back to 1950, when Grupe and Warren proposed the technique achieving a predictability of root coverage between 65 % and 75 %. On the other hand, among its limitations, it was inadequate in cases with a shallow vestibule or insufficient gingival dimensions lateral to the recession site.(47)
Nelson, in 1987, described a full-thickness double papilla flap to cover the connective tissue graft. This method was modified in 1992 by Harris using a split-thickness double papilla flap and in a subsequent publication, the same author reported the use of the technique in 100 consecutively treated defects with an average root coverage of 97,1 %.(48,49)
Blanes describes in his article the bilateral tunnelled pedicle flap as a technique that provides vascular supply to compensate for the lack of blood supply in deep or wide adjacent recessions. In the first stage, the recipient site is prepared by making a partial-thickness flap, preserving the papilla medial to both recessions. Horizontal incisions are placed at the level of the cemento-adamantine junction. The vertical incisions at the end of the horizontal incisions extend approximately 10 to 12 mm apically. Partial thickness lateral pedicle flaps are reflected without disturbing the interproximal papilla in the midline. In the second stage, the graft is placed and sutured with single sutures apically and corally. Also, suspensory sutures can be used to secure the graft coronally. Finally, the lateral pedicle flaps are rotated mesially and sutured over the facial aspect of the roots with suspensory sutures. The mesial edges of the lateral pedicle flaps can be sutured to the interproximal papilla with simple sutures.(48)
Espinel, on the other hand, describes the laterally positioned pedicle technique where the flap is elevated from the donor site as partial thickness, then divided into total thickness proximal to the recession, and finally displaced laterally.(49)
The surgical technique is as follows: First, the tissue collar around the recession is removed through two vertical incisions that meet at an apical point at the base of the recession. The incision corresponding to the side from which the lateral flap will be moved bevelled internally. The opposite collar of tissue was removed through a wide incision bevelled externally. This arrangement allows the lateral flap to be superimposed over a vast bed of fresh connective tissue once it is sutured into position. Another vertical incision is made away from the recession, including the papilla, and extended beyond the alveolar mucosa through an oblique release incision to provide adequate flap mobility.
The flap was separated as follows: Half of the flap away from the recession was reflected as partial thickness, then half of the flap close to the recession was made total thickness. The whole flap was finally released by making an incision through the periosteum at its apical base. Free of tension, the flap is passively placed on the prepared root surface.
The internally bevelled edge of the flap overlaps the externally bevelled recipient edge by suturing the margins with a single suture. An additional suture is placed to stabilize the flap in the donor area, which is left protected by the periosteum. The sutures are removed after one week.(48)
Zucchelli, in 2004, describes a modified surgical approach to the original laterally displaced flap procedure for the treatment of single recessions, combining the aesthetic and root coverage advantages of the advanced coronary flap with the increased gingival thickness and keratinized tissue associated with the laterally displaced flap technique.(26)
The procedure is described in two stages: the preparation of the recipient area and the design of the flap itself. Initially, the recipient area is prepared by deep triangular de-epithelialization delimited by three incisions. A first horizontal incision 3mm extended in a mesial-distal direction at the level of the LAC, a second bevelled vertical incision parallel to the mesial gingival margin of the recession extending into the alveolar mucosa and a third bevelled intra-crevicular incision along the distal gingival margin of the recession defect extending into the alveolar mucosa until crossing with the second incision.
The design of the flap to be mobilized consists of three incisions. The first one is infraclavicular bevelled equal to the last incision of the recipient area. The second incision is made horizontally submarginally, extending in a mesiodistal direction 6mm wider than the width of the recession defect measured at the LAC. At this point, the author makes an observation that varies depending on the need to preserve at least 1mm of keratinized tissue of the donor tooth along the mesiodistal extension of the flap. If the probing depth is less than 1mm, a height of 3mm of donor tissue should be planned, while in the presence of a 2mm donor tissue, at least 4mm of keratinized tissue is required. Finally, the third bevelled oblique vertical incision is made, extending into the mucosa parallel to the first crevicular incision. When the flap is mobilized in the mesial direction, another short horizontal incision is made at the most apical extension of the flap to facilitate the mesial movement.(26)
All muscle insertions were removed to allow coronal advancement of the flap. The remaining epithelial tissue of the anatomic interdental papillae was de-epithelialized to create connective tissue beds to which the surgical papillae of the coronally displaced flaps were sutured.(26,47)
The synthesis begins by performing two simple periosteal sutures at the most apical extent of the vertical release incisions, then advances coronally along the vertical mesial incision, with further simple sutures, each directed from the flap to the adjacent vestibular soft tissue in an apical-coronal direction. More apically, a horizontal double mattress suture is performed to reduce lip tension on the marginal portion of the flap. After these sutures, the more marginal portion of the flap was held stable in the coronal position with a suspensory suture. The coronally positioned flap has been suggested to treat localized gingival recessions without disturbing adjacent teeth.(47) The reason for the lack of interest in pedicled techniques relates to the fact that the data do not seem to indicate that this technique achieved highly predictable and effective root coverage, with the coronal repositioning flap being the treatment of choice for localized gingival recessions, without disturbing the margins of adjacent teeth.(26,47,48)
Tunnel techniques
In 1999, Zabalegui et al. connected the mesial and distal multiple envelopes without detaching the papilla by forming a mucosal tunnel, creating the tunnel technique. It is based on constructing a tunnel under the gingival tissue consisting of a sulcular incision beyond the mucogingival line without lifting the papilla. A large connective tissue graft from the palate is introduced through the tunnel to cover the adjacent gingival recessions. This technique allows the treatment of multiple adjacent gingival recessions in a single procedure with adequate early healing and highly predictable coverage results.(50)
The procedure begins by making partial-thickness intracellular incisions, preserving the papilla, undermining the tissue coronal to the amelocemental boundary until it overpasses the mucogingival line; the dissection extends laterally through the papilla between the teeth, remaining intact. A connective tissue graft is then harvested and placed in the recipient bed using vertical mattress sutures.(51)
Zuhr et al. 2007 reevaluated the tunnel technique since it was mentioned as a complex approach and sensitive to the operator’s hand, having to maintain a uniform thickness over the periosteum for the correct sliding of the graft into the recipient bed. Thus, advances in microsurgery introduced new instruments to minimize trauma and ensure a better blood supply to the graft.(50)
The technique described by the author begins by making intracellular incisions around the affected tooth necks using a micro-scalpel blade, which has blades on both sides and at the tip, followed by the collaboration of the tunnelers, the latter have different working angles allowing access in the anterior sector saving the convexity of the vestibular faces. The undercut is extended to the mucosa, and each access is connected at partial thickness, allowing the connective tissue graft to be placed. Once the connective tissue graft is placed using vertical mattress stitches, a mattress suture is performed starting from the palatal area, allowing the coronal mobilization of the tissues. The suture should take the vestibular flap and the subepithelial connective tissue to stabilize the CTG.
In 2010, Aroca published the modified coronal advancement tunnel technique for treating multiple Miller class III recessions, using composite stitches in the interproximal areas to maintain the position of the tissue during healing using horizontal mattress stitches with a loop.(52) The surgical approach begins with an acid etching technique, adhesive and composite stitches at the level of the contact points. Then, a full-thickness intracellular incision is made above the recessions, advancing with tunnelers until the mucogingival line is surpassed. Once the bed has been achieved in a uniform way that allows the displacement without tension, the graft is introduced through the most expansive recession area using a mattress suture, and finally, the flap is displaced with horizontal mattress sutures with loop.(52)
Laterally positioned flap with stretching (LAST)
Carranza, in 2019, presented an alternative treatment to the traditional lateral displaced flap procedure and tunnelling techniques commonly used for the coverage of deep and narrow recessions, the “Lateral flap with stretching” with a connective tissue graft. Treating this type of recession with displaced flaps improves the nutritional supply versus no vertical incisions while producing a more stable wound with minimal scarring and less discomfort for the patient.(53)
The following is the step-by-step surgical technique: Intra-crevicular incisions are made involving the tooth with the recession and at least one adjacent tooth on each side. Then, a partial thickness envelope flap is prepared with tunnelers extending the bed 1 or 2 adjacent teeth. In areas with a thin phenotype, a full-thickness flap will be made. On the other hand, the technique presented can be modified by two horizontal incisions described by Bruno, allowing the graft to be placed in a more coronal position and improving access and visibility. A connective tissue graft is taken with a double scalpel blade technique extending 5mm on each side and 5mm apical to the deepest recession. The graft is placed in the recipient bed and held by mattress sutures on both sides of the envelope. Then, the lateral edges of the recession are approximated with simple sutures without taking the underlying graft to cover the graft, minimizing exposure and stabilizing the wound.(53)
Vestibular Incision Subperiosteal Tunnel Access Technique (VISTA)
Zadeht introduces a novel and minimally invasive approach applicable for both isolated recession defects and multiple defects in the maxillary anterior region by obtaining access to the surgical site through an approach called subperiosteal tunnel access via vestibular incision, decreasing the associated morbidity and minimizing scar formation at the recipient site.(54)
As we have been reviewing in the tour of current techniques, tunnel preparation uses an intracellular approach to create a subperiosteal space that extends beyond the mucogingival junction, allowing the graft tissue to be inserted beneath the gingival collar. Limitations of this tunnel access technique include the technically challenging nature of the bony anatomy due to the small marginal access point and the increased risk of traumatizing and perforating the sulcular tissues, potentiating possible unfavourable healing outcomes. Due to these limitations, the vestibular incision subperiosteal tunnel access approach (VISTA) was developed to avoid potential complications of intracellular tunnelling techniques. The technique proposes to make an access incision in the upper anterior frenulum followed by elevation of a subperiosteal tunnel. However, the location of the access incision depends on the sites to be treated. This tunnel extends at least one or two teeth beyond the root recession to mobilize the gingival margins and facilitate coronal repositioning. Moreover, it is essential to extend the elevation sufficiently beyond the mucogingival margin and across the gingival sulci of the teeth to be augmented to allow for low-stress coronal repositioning of the gingiva. In addition, the subperiosteal tunnel is extended in the interproximal area below each papilla as far as the pocket space allows without making superficial incisions through the papillae. Once the bed is created, a connective tissue graft or collagen membrane is placed, and suturing is performed by introducing a new method of stabilizing the gingival margins, called coronally anchored suture, designed to maintain the coronal position of the gingival margins during healing.(54)
Decision-making flow chart for single and multiple recessions in the upstream industry
To consider the appropriate technique for each clinical case, we must first consider eliminating any inflammatory state by performing essential therapy, leaving a surface compatible with health without pocket depth or bleeding.(16)
From a topographical point of view, the presence of non-carious cervical lesions should be considered by a combined restorative/periodontal treatment facilitating the reconstruction of the amelocemental boundary, providing a smooth, stable and convex surface for the surgical flap.(55)
The relationship between gingival recession and orthodontic treatment is widely described in the literature, which is why it is essential to manage the patient concomitantly between the periodontist and the orthodontist, even more so if the pathology exists before corrective treatment is started. In cases where the orthodontic treatment undergoes poor clinical management, the periodontal tissues are highly affected, and the prognosis worsens if the treatment is not adequately followed up.(30)
The amount of gingiva inserted to maintain the health and stability of the gingival margin can be less than 2mm, as long as there is good oral hygiene. Many studies conclude that using surgical procedures to increase the band of keratinized gingiva is questionable.(23)
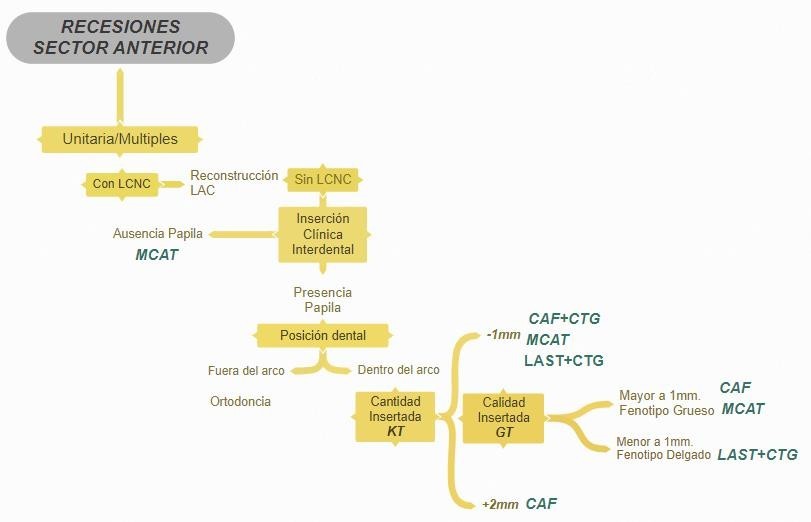
Figure 1. Flowchart for decision-making in the treatment of upstream recessions. References: CNCL, non-carious cervical lesion. LAC, amelocemental border. KT, Keratinized tissue. GT, gingival thickness. MCAT, Modified coronal advancement tunnel. CAF, Coronal advancement flap. CTG. Connective tissue graft. LAST, Lateral advancement technique with stretching.
CONCLUSIONS
The results of the theoretical discussion affirm that the selection of one surgical technique over another depends mainly on the local anatomical characteristics of the site to be treated and secondarily on the aesthetic demands of the patient, taking relevance at the moment of defining the approach.
On the other hand, clinical aspects and customization of the treatment plan according to each patient’s specific needs are essential to ensure a comprehensive and interdisciplinary approach that collaborates with the periodontist to achieve successful root coverage that improves esthetics and long-term periodontal health.
The literature review concludes that periodontal health can be maintained in most patients even with minimal amounts of keratinized tissue. However, gingival recession is typical in thin periodontal phenotypes, poor oral hygiene or orthodontic treatment. Aesthetic concerns, hypersensitivity and related alterations in health parameters are addressed with mucogingival surgical interventions to prevent or treat recessions.
Miller Class I and II recessions are the most predictable for root coverage, while Classes III and IV require more planning and professional expertise. Several surgical techniques, from free grafts to coronal advancement tunnels, seek to improve periodontal health and esthetics, considering the individual needs of each patient and the interdisciplinary collaboration of the different specialities in dentistry.
The decision-making flow chart includes the following axes: single or multiple recession, depth and type of recession, level of clinical interdental insertion, amount of inserted gingiva and quality of gingival tissue.
REFERENCES
1. Serino G, Wennström J, Lindhe J, Eneroth L. The prevalence and distribution of gingival recession in subjects with a high standar or oral hygiene. J Clin Periodontol 1994;21:57-63.
2. Brito Pérez K, Cruz Morales R, Caballero López D. Trastornos mucogingivales y su tratamiento, cinco años de seguimiento en pacientes matanceros. Rev Medica Electron 2017;39:269-79.
3. Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: a systematic review. J Clin Periodontol 2008;35:136-62.
4. Corrales I, Palacio P, Arango R. Estado actual del manejo de recesiones gingivales mediante cirugía plástica periodontal. Rev CES Odontol 2009;22:57-66.
5. Miller P. Injerto de cobertura radicular para regeneración y estética. Periodontology 2000;1:118-27.
6. Pini-Prato G. Clasificación de recesiones gingivales de Miller. Límites y desventajas. J Clin Periodontol 2011;38:243-5.
7. Cairo F. El nivel de inserción clínica proximal para la clasificacion y predicción de cobertura radicular. J Clin Periodontol 2011:661-6.
8. Sociedad Argentina de Periodontología. Clasificación de las enfermedades y alteraciones periodontales y periimplantares 2017 AAP-EFP 2017.
9. Zucchelli G, Mounssif I. Cirugía plástica periodontal. Periodontol 2015;68:333-68.
10. Afanador Ruiz C, Duque Naranjo C, Gómez de Ramírez C. Historia de la periodoncia: primeros rasgos de definición de un espacio social y conceptual y proceso de institucionalización en Colombia. parte I. Una imagen de la periodoncia a través de su historia y de su historiografía. Rev Colomb Filos Cienc 2004;3:77-103.
11. Friedman N, Levine L. Cirugía mucogingival: estado actual. En Annu. Meet. Am. Acad. Periodontol. AAP Internet, Ciudad Nueva York: AAP Academia Americana de Periodoncia; 1964, p. 5-21. https://doi.org/10.1902/jop.1964.35.1.5.
12. Lindhe J, Karring L, N. Periodontología Clínica e Implantología Odontológica. 5.a ed. Buenos Aires, Argentina: Panamericana; 2009.
13. Chambrone L, Sukekava F, Araújo M, Pustiglioni F, Chambrone LA, Lima L. Procedimientos de cobertura de raíces para el tratamiento de defectos localizados de tipo recesión: una revisión sistemática Cochrane. J Periodontol 2010;81:452-78.
14. Kan J, Morimoto T. Evaluación del biotipo gingival en la zona estética: inspección visual frente a medición directa. Int J Restor Dent Periodontics 2010;14:237-43.
15. Cortellini P, Bissada N. Condiciones mucogingivales en la dentición natural: revisión narrativa, definiciones de casos y consideraciones diagnósticas. J Periodontol 2018;89.
16. Stefanini M, Aroca S, Zucchelli G. Toma de decisiones en procedimientos de cobertura radicular para el resultado estético. Periodontology 2000;77:54-64.
17. Ardila Medina C. Recesión gingival: una revisión de su etiología, patogénesis y tratamiento. Av Periodoncia 2009;21:35-43.
18. Litonjua L, Andreana S, Bush P, Cohen R. Cepillado y recesion gingival. Int Dent J 2003;53:67-72.
19. Injante Ormeño P, Tuesta Da Cruz O, Estrada Vitorino M, Liñán Durán C. Recesión gingival y tratamiento de ortodoncia. Reporte de un caso interdisciplinario. Rev Estomatol Hered 2012;22:31-6.
20. Leal L. La correlación entre el fenotipo gingival y la forma dentaria en los pacientes adultos. Tesis de grado para optar por el título de Odontologo. Universidad Abierta Interamerincana, 2021.
21. Susin C, Haas A, Oppermann R, ola H, Albandar J. Recesión gingival: epidemiología e indicadores de riesgo en una población urbana representativa de Brasil. J Periodontol 2004;75:1377-86.
22. Yadav VS, Gumber B, Makker K, Gupta V, Tewari N, Khanduja P. Prevalencia global de recesión gingival: una revisión sistemática y un metanálisis. Oral Dis 2023;29:2993-3002.
23. Tonetti M, Jepsen S. Eficacia clínica de los procedimientos de cirugía plástica periodontal: Informe de consenso del Grupo 2 del 10o Taller Europeo de Periodoncia. J Clin Periodontol 2014;41:36-43.
24. Pini-Prato G, Tinti C, Vincenzi G, Magnani C, Cortellini P, Clauser C. Regeneración tisular guiada versus cirugía mucogingival en el tratamiento de la recesión gingival bucal humana. J Periodontol 1992;63:919-28.
25. Ronco V. Tunneling. A Comprehensive Concept in Periodontal Plastic Surgery. 1.a ed. Croatia: Quintessence Publishing Co; 2022.
26. Zucchelli G, Cesari C, Amore C, Montebugnoli L, Sanctis M. Colgajo coronalmente avanzado y movido lateralmente: un abordaje quirúrgico modificado para defectos aislados de tipo recesión. J Periodontol 2004;75:1734-41.
27. Langer B, Langer L. Técnica de injerto de tejido conectivo subepitelial para cobertura de raíces. J Periodontol Diciembre De 1985;56:715-20.
28. Echeverría J, Manau C. Injertos Gingivales Libres. Arch Odonto-Estomatol 1989;5:388-94.
29. Sarduy Bermúdez L, Corrales Álvarez M. Injerto libre de encía en el tratamiento de la recesión periodontal. Medicent Electrón 2014;18:135-9.
30. Vicario-Juan M. Técnicas de cirugía mucogingival para el cubrimiento radicular. RCOE Rev Col Odontol Estomatol Esp 2006;11:61-73.
31. Tarnow D, Fletcher P, Magner A. El efecto de la distancia desde el punto de contacto hasta la cresta ósea sobre la presencia o ausencia de la papila dental interproximal. J Periodontol 1992;995-6.
32. Allen A. Uso de la envoltura supraperióstica en injertos de tejidos blandos para cobertura radicular. I. Racional y Tectinica. Int J Periodontics Restor Dent 1994;14:217-27.
33. Cavenaghi G, Caccianiga G, Baldoni M, Lamedica M. Comparación entre técnicas bilaminares y regenerativas para recubrir las raíces. Av Periodoncia 2000;12:127-36.
34. Ariceta A, Viera Mendez F, Velasquez D. Comparación de tomas de injertos de tejidos blandos: Una revisión narrativa. Int J Interdiscip Dent 2022;15:165-8.
35. Zuhr O, Bäumer D, Hürzeler M. La incorporación de injertos de reemplazo de tejido blando en cirugía plástica periodontal e implantología: elementos críticos en el diseño y ejecución. J Clin Periodontol 2014;41.
36. Harris R. Comparación de dos tectiniques para la obtención de un injerto de tejido conectivo del paladar. Int J Periodontics Restor Dent 1997;17:261-71.
37. Bruno J. Técnica de injerto de tejido conectivo que garantiza una amplia cobertura radicular. Int J Periodontics Restor Dent 1994;14:127-37.
38. Hürzeler M, Weng D. Técnica de insición única opara recolectar injertos de tejido conectivo subepitelial del paladar. Int J Periodontics Restor Dent 1999;19:279-87.
39. Zucchelli G, Mele M, Stefanini M, Mazzotti C, Marzadori M, Montebugnoli L. La morbilidad del paciente y el resultado de la cobertura radicular después de la toma de tejido conjuntivo subepitelial o injertos desepitelializados: un ensayo clínico controlado aleatorizado comparativo. J Clin Periodontol 2010;37:728-38.
40. Carranza Cholán L, Mantilla Gil M. Estudio comparativo entre el cepillo ecológico y el cepillo de plástico en la eliminación de la placa bacteriana en estudiantes de una Institución Educativa Cajamarca, 2019. Universidad Privada Antonio Guillermo Urrelo, 2020.
41. Reiser G, Bruno J, Mahan P, Larkin L. El sitio donante palatino del injerto de tejido conectivo subepitelial: consideraciones anatómicas para los cirujanos. Int J Restor Dent Periodontics 1996;16:130-7.
42. Tavelli L, Barootchi S, Ravida A, Oh TJ, Wang HL. ¿Cuál es la zona de seguridad para la extracción de injertos de tejido blando palatino según la ubicación de la arteria y el agujero palatino mayor? Una revisión sistemática. J Oral Maxillofac Res 2018;77:1-9.
43. Sanz I. Diferencias estructurales e histológicas entre injertos de tejido conectivo obtenidos de la mucosa palatina lateral o del área de la tuberosidad. Clin Oral Investig 2018;1.
44. Studer S, Allen E, Rees T, Kouba A. El espesor de la mucosa masticatoria en el paladar duro y la tuberosidad humanos como posibles sitios donantes para procedimientos de aumento de crestas. J Periodontol 1997;68:145-51.
45. Sanctis M, Zucchelli G. Colgajo desplazado coronalmente: un abordaje quirúrgico modificado para recesiones unitarias. J Clin Periodontol 2007;34:262-8.
46. Zucchelli G, Stefanini M, Ganz S, Mazzotti C, Mounssif I. Colgajo coronalmente avanzado con diferentes diseños en el tratamiento de la recesión gingival: un ensayo clínico aleatorizado controlado comparativo. Int J Periodontics Restor Dent 2016;36:319-27.
47. Zucchelli G, Marzadori M, Mele M, Stefanini M, Montebugnoli L. Cobertura radicular en molares: un ensayo clínico aleatorizado controlado comparativo. J Clin Periodontol 2012;39:1082-8.
48. Blanes R, Allen E. La técnica del túnel del colgajo pedicular bilateral: un nuevo enfoque para cubrir los injertos de tejido conectivo. Int J Periodontics Restor Dent 1999;19:471-9.
49. Espinel M, Caffesse R. Colgajo posicionado lateral, técnica de aleta deslizada revisada en el tratamiento de las recesiones gingivales localizadas. Int J Periodontics Restor Dent 1981;1:42-51.
50. Zuhr O, Fickl S, Wachtel H, Bolz W, Hürzeler MB. Covering of gingival recessions with a modified microsurgical tunnel technique: case report. Int J Periodontics Restorative Dent 2007;27:457-63.
51. Zabalegui I, Sicilia A, Cambra J, Gil J, Sanz M. Tratamiento de múltiples recesiones gingivales adyacentes con el injerto de tejido conectivo subepitelial en túnel: informe clínico. Int J Periodontics Restorative Dent 1999;19:199-206.
52. Aroca S, Keglevich T, Nikolidakis D, Gera I, Nagy K, Azzi R, et al. Treatment of class III multiple gingival recessions: a randomized-clinical trial. J Clin Periodontol 2010;37:88-97. https://doi.org/10.1111/j.1600-051X.2009.01492.x.
53. Carranza N, Pontarolo C, Rojas M. Laterally stretched flap with connective tissue graft to treat single narrow deep recession defects on lower incisors. Clin Adv Periodontics 2019;9:29-33.
54. Zadeh H. Tratamiento mínimamente invasivo de los defectos de recesión gingival anterior del maxilar mediante acceso al túnel subperióstico por incisión vestibular y factor de crecimiento derivado de plaquetas BB. Int J Periodontics Restorative Dent 2011;31:1-9.
55. Zucchelli G, Gori G, Mele M, Stefanini M, Mazzotti C, Marzadori M. Lesiones cervicales no cariosas asociadas con recesiones gingivales: un proceso de toma de decisiones. J Periodontol 2011;82:1713-24.
FINANCING
The authors did not receive funding for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Ianina Solange Silvera.
Data curation: Ianina Solange Silvera.
Formal analysis: Ianina Solange Silvera.
Research: Ianina Solange Silvera.
Methodology: Ianina Solange Silvera.
Project administration: Ianina Solange Silvera.
Resources: Ianina Solange Silvera.
Software: Ianina Solange Silvera.
Supervision: Ianina Solange Silvera.
Validation: Ianina Solange Silvera.
Visualization: Ianina Solange Silvera.
Writing - original draft: Ianina Solange Silvera.
Writing - proofreading and editing: Ianina Solange Silvera.